Government health spending in India
Published on June 12, 2022
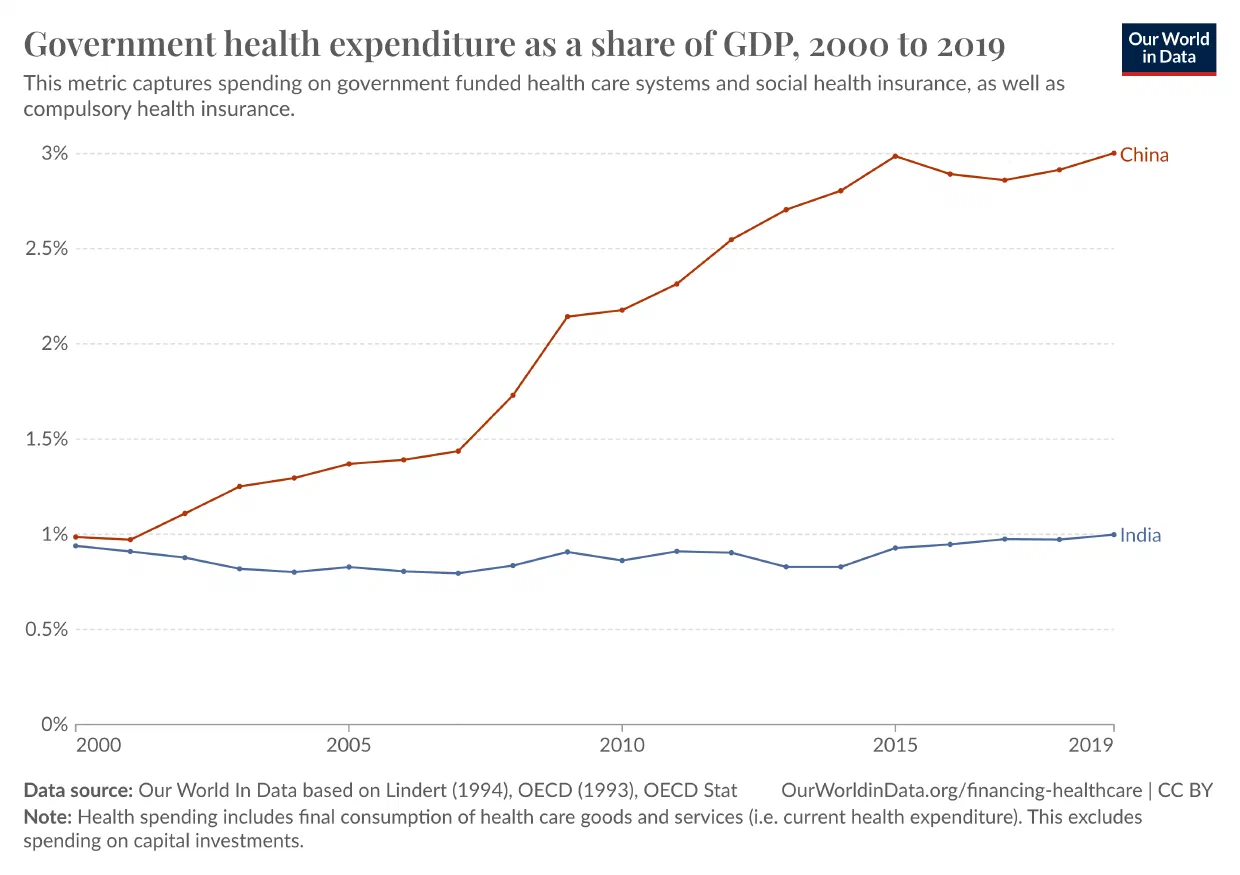
This is a strange graph. Usually, governments spend more on healthcare as they become richer. Between 2000-2018, India’s GDP grew from $468 billion to $2.7 trillion. In the same period, Chinese Government Health Spending (GHS) grew from one percent to nearly three percent of GDP. In India, however, GHS stagnates at around one percent. Relative to GDP, India has one of the lowest public health budgets in the world.
Government health spending (the Union and the States combined) makes up less than a third of total health expenditure in India. And formal insurance schemes make up less than a tenth. Most healthcare costs are paid by patients out of pocket, and most of that goes to medicines, diagnostics, and outpatient care.
Why isn’t more money going to health? Health and education, Amartya Sen keeps telling us, are central to sustained economic growth.1 This is, of course, a product of the slightly important fact that people end up living longer, healthier lives. Why wouldn’t India want a thriving, healthy middle class and profit from that demographic dividend everyone keeps talking about?
Potential Causes
One explanation is that healthcare, as an issue, has not become a persistent electoral demand.2 While India is not particularly spendthrift – government spending was only about 18% of GDP in 2021 – we are capable of significant social spending when the electoral incentives align, such as when we fund massive food and fertiliser subsidies to “cushion the pain” as the Indian economy went through structural transformation. In healthcare, there hasn’t been a huge electoral incentive to spend on health.
After independence
The Congress party was committed to social spending and enjoyed unparalleled electoral dominance. Sujatha Rao’s Do We Care? (2016), which we will rely on extensively, blames economists for this. The post-independence Nehruvian Model emphasised economic planning and development, and particularly focused on self-sufficiency and reducing imports. The government focused aggressively on irrigation, agriculture, and power plants and neglected education and health in the process. While China was launching massive campaigns for behaviour change, hygiene, and sanitation, India stuck to a narrow public health agenda limited to family planning and malaria prevention.
After liberalisation
The private sector can provide healthcare, and they fill a massive gap in healthcare provision, but not at a low enough cost to meet the needs of India’s poorest. And the private sector can’t do massive public health programmes or invest in preventive care. But this isn’t a reason to discount them entirely.
Contrary to popular perception, private healthcare is not merely available to the wealthy. In rural India, “most providers are in the private sector (86 per cent)”, though they are not what one imagines when one pictures expensive private hospitals. These private providers are usually unqualified – with no formal training. However, it turns out (from a 2010-11 study in rural Madhya Pradesh and urban Delhi) that “private practitioners with no formal training were as likely to diagnose correctly as qualified doctors in government hospitals.” But if government doctors are as bad as unqualified providers, that might as well be a failure of medical education, not the success of the market.
Why haven’t the States invested heavily in healthcare?
Some have, and they’re mostly southern states like Kerala and Tamil Nadu. You can’t give social democracy all the credit - these states had serious advantages and still incurred serious costs. Most people in Kerala are in small towns which are somewhat proximate to each other, making it much easier to get over physical distance and reducing inequalities between urban and rural areas, one of the biggest barriers to healthcare access. Kerala’s government was willing to throw out fiscal discipline, take on debt, and aggressively invest in people’s well-being all the way until they ended up in a multi-decade fiscal crisis. By that point, however, infrastructure had developed sufficiently, an epidemiological transition had taken place, and the private sector could take it from there.
Poverty
In some states, like Bihar or Uttar Pradesh, the answer is just poverty. On average, according to Rao, states need to “almost treble their spending from the current level of 2.4% to 8%.” This is difficult, because the states that are bad at public health also don’t have enough money. Rao writes: “Three-quarters of disease burden is concentrated in about nine states that also account for an equal number of the poor.” Additionally, the “per capita income ratio between them and the better-off states is 1:5, making it impossible for any central government to bridge the divide.” Those who most need to spend cannot and those who can really don’t need to.
You simply cannot get around poverty. You cannot redistribute your way out of your problems unless you get to a minimum level of GDP-per-capita. Whatever that minimum is, it’s higher than Uttar Pradesh’s measly $860. For reference, the Indian average in 2019 was $2100 and Kerala’s in 2021 was $3100. Rao says that the capital investment necessary to bridge this gap would require a hike in the tax-to-GDP ratio by at least 20 percent. And the government can’t raise taxes or introduce copayments or fees because almost everyone (93%) works in the informal sector and about 40% of them have “no assets or steady incomes.” There’s also an enormous failure of medical education. Credentials are not predictors of quality in poorer states: qualified doctors in Bihar scored lower than unqualified providers in Kerala.
Division of powers
Rao blames the federal division of powers for this. While the States and the Union can both legislate on relatively inexpensive areas like drug regulation or statistical collection, only the States are empowered to deal with public health, sanitation, hospitals, and dispensaries. This division of powers condemns the States to perpetual fiscal insecurity and makes them dependent on the Union for grants. Some revenues are collected by the Union and shared with the States, and the precise split is managed by the Finance Commission, which has almost never made health a priority. If the Union doesn’t make health a priority, the States will have to do so. And as we have seen, there are various reasons why the States can’t, or at least find it difficult.
Organisational capacity
Indian bureaucracies, notorious for their centralisation and slowness, delay the release of funds and withhold approved budgets. Rao describes, with evident frustration, how short-termism is baked into the operating protocols of the Indian state. In some instances, approval would be granted by a bureaucrat who would, minutes later, call up the finance department and tell them not to sanction the necessary funds.
Conclusion
To sum up, It’s not just expensive, but also incredibly hard to spend on health in a way that moves the needle. Policymakers and administrators face a complex, labyrinthine bureaucracy, as well as an inflexible constitutional structure that is allergic to long-term thinking. These factors condemn parts of India to generational poverty, illiteracy, and ill health.
Pradyumna Prasad, Akshay, Nithya, Akshay Dinesh, and Sanjana reviewed early drafts and improved this post substantially with their helpful comments.
If I haven’t linked to a fact or statistic in the body text, it’s from one of the following books:
- Rukmini S., Whole Numbers and Half Truths: What Data Can and Cannot Tell Us About Modern India (2021) (amazon)
- Sujatha Rao, Do We Care? India’s Health System (2018) (amazon)